Introduction
Hospital bed casters rank among the most heavily stressed components in any clinical setting. They support patient weight exceeding 400 pounds, endure dozens of repositioning cycles daily, and face constant exposure to disinfectants, floor transitions, and emergency maneuvers.
Replace them too late, and you're looking at failed safety inspections, staff injury claims, and unplanned bed downtime — all preventable.
Between 700,000 and 1 million hospitalized patients fall each year, with more than one-third resulting in injury. Equipment stability—including bed brake and caster integrity—represents a controllable variable in fall prevention programs. The risk extends to staff as well. Nursing assistants experience an MSD incidence rate of 166.3 per 10,000 workers, more than five times the all-industry average, with degraded casters compounding push-pull force requirements throughout every shift.
This guide covers the warning signs of caster failure, how replacement timing varies by facility type and usage intensity, and what to evaluate when selecting replacements that maintain compliance with IEC 60601-2-52 bed safety standards.
Key Takeaways
- Timely replacement prevents patient falls, staff injuries, floor damage, and compliance citations
- Replace casters when treads crack or flat-spot, bearings grind, brakes slip, or housings show corrosion
- Inspection frequency depends on usage: high-acuity units every 3 months, lower-traffic areas every 6-12 months
- Match load rating, wheel material, and mount type to the specific bed model and floor surface
- Scheduled replacements cost far less than emergency sourcing or incident liability after a visible failure
Why Timely Caster Replacement Matters in Healthcare Settings
Hospital bed casters operate under conditions that accelerate wear far beyond typical industrial applications. Standard pressure injury prevention protocols recommend patient repositioning at minimum every 2 hours, translating to 12 bed-movement events daily for repositioning alone. That figure excludes transport to imaging, transfers to surgical tables, bedside procedures, and terminal cleaning cycles between patient discharges.
Patient Safety Impact
Worn casters increase the risk of unexpected bed movement during transfers, a leading contributor to patient fall incidents. The AHRQ PSNet database documents fall rates of 3-5 per 1,000 bed-days, with CMS classifying falls resulting in serious injury as non-reimbursable "never events." A caster brake that fails to engage during a lateral transfer removes a critical safety margin precisely when patient vulnerability peaks.
The Joint Commission classifies death or serious injury from falls as sentinel events requiring root cause analysis. While comprehensive data isolating caster-specific contributions to fall incidents remains limited, accreditation surveyors evaluate equipment safety and preventive maintenance programs under Environment of Care standards (EC.02.04.01). Documented caster failures on patient transport equipment can trigger citations or corrective action plans.
Staff Ergonomics and Injury Risk
Degraded casters raise rolling resistance, meaning nurses and aides exert greater push-pull force throughout their shifts. This compounds fatigue and elevates musculoskeletal injury risk in an already high-risk occupation. U.S. hospitals recorded 7.6 work-related injuries per 100 full-time employees in 2020 (nearly three times the all-industry rate of 2.7).
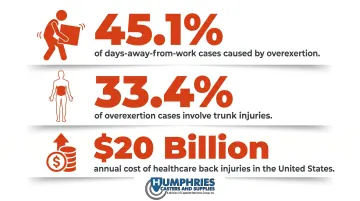
The downstream costs are substantial:
- Overexertion causes 45.1% of all cases with days away from work in private hospitals
- Trunk injuries account for 33.4% of those overexertion cases
- OSHA estimates back injuries in healthcare cost approximately $20 billion annually in direct and indirect expenses
Compliance and Accreditation Exposure
CMS Survey & Certification Letter 14-07 permits hospitals to adjust preventive maintenance frequencies using risk-based assessment, but prohibits deviation from manufacturer recommendations for equipment without sufficient maintenance history. Facilities must document and justify inspection schedules, with equipment maintenance consistently appearing as a top area of Joint Commission non-compliance.
Warning Signs Your Hospital Bed Casters Need Replacing
Wheel Tread Degradation
Healthy caster treads appear smooth and uniform. Replace immediately when you observe:
- Cracking or surface fissures, which signal material fatigue and imminent tread separation
- Flat spots from prolonged stationary loading, creating vibration patients feel during transport
- Chunking where missing tread sections expose core materials and accelerate bearing damage
- Surface hardening that turns rubber glossy and rigid, eliminating shock absorption and increasing noise
Each condition impairs smooth movement and creates uneven load distribution across remaining casters, accelerating their failure.
Bearing Failure Indicators
A caster in good condition rolls nearly silent. Any of these sounds during movement warrants inspection:
- Grinding or squealing during straight-line movement
- Clicking sounds during swivel rotation
- Uneven rolling resistance requiring compensatory pushing
- Visible wobble when the bed is stationary
These signals indicate internal bearing wear. Staff often unconsciously push harder to compensate, accelerating damage to both the failing caster and the remaining casters now carrying extra strain.
Brake and Locking System Malfunction
Test both failure modes during inspection:
- Brake won't engage: beds drift during patient transfers, creating immediate fall risk — even partial slippage under load constitutes failure
- Brake won't release: forces staff to rock beds free or apply excessive force, damaging floor surfaces and caster housings
- Central locking failure: if even one of four casters doesn't respond to the pedal, the entire bed is unsafe for transfers
Central locking systems, common in acute care beds, carry more mechanical stress points than simple swivel brakes and require earlier inspection intervals.
Structural and Hardware Issues
Physical inspection should identify:
- Bent or cracked housing assemblies
- Wobbly or loose stems indicating mount degradation
- Corroded fasteners, particularly in high-humidity environments
- Visible cracks in the caster frame itself
- Missing or damaged electrical grounding chains
High-humidity environments like ICU corridors, cleaning areas, and rooms with frequent washdowns accelerate corrosion beyond normal timelines.
Hygiene and Infection Control Failures
Damaged seals, pitted wheel surfaces, or corroded crevices trap disinfectant residue and biofilm, making thorough cleaning impossible. The CDC classifies hospital bed casters as noncritical equipment surfaces requiring low-level disinfection with EPA-registered hospital disinfectants.
When caster surfaces degrade to the point where recommended cleaning protocols cannot reach all surfaces, replacement becomes a mandatory infection control requirement regardless of mechanical function.
When to Replace: Timing Based on Usage Load, Environment, and Condition
No single replacement interval works for every facility. Timing depends on usage intensity, floor conditions, environmental factors, and bed type. CMS permits risk-based maintenance scheduling, but facilities must document inspection findings and replacement rationale.
Based on Usage Volume and Bed Location
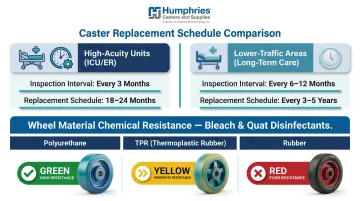
High-acuity environments (ICU, ER, surgical units):
- Beds move constantly for procedures, imaging, and patient transfers
- Casters experience maximum mechanical stress
- Inspection recommended every 3 months
- Replace within 18-24 months of heavy use
Lower-traffic areas (long-term care, post-acute wards):
- Beds reposition primarily for patient comfort and cleaning
- Reduced frequency allows longer service life
- Inspection recommended every 6-12 months
- Replace after 3-5 years
Beds with central locking casters have more mechanical stress points than simple swivel casters. The locking mechanism itself—connecting all four casters to a single pedal control—requires earlier inspection intervals than non-linked systems.
Based on Environmental and Chemical Exposure
Floor surface is a major wear accelerator, independent of how often a bed moves:
- Abrasive surfaces (textured safety flooring, aggregate-finish epoxy)
- Uneven transitions between carpet and tile
- Door thresholds and elevator gaps
- Debris accumulation in high-traffic corridors
Beyond floor wear, cleaning chemistry puts its own stress on caster materials. Polyurethane demonstrates good resistance to bleach (sodium hypochlorite) at standard dilutions, while natural/synthetic rubber shows poor resistance, experiencing chalking, brittleness, and cracking. TPR (thermoplastic rubber) offers moderate resistance between the two.
Facilities using aggressive cleaning protocols—including quaternary ammonium compounds or bleach-based disinfectants applied multiple times daily—should shorten replacement cycles and favor polyurethane over rubber-based treads.
Based on Planned Maintenance Windows vs. Reactive Failure
Preventive replacement occurs during scheduled maintenance downtime, aligned with equipment servicing rounds. Benefits include:
- Controlled procurement timelines with competitive pricing
- Installation during low-census periods
- Batch replacement ensuring matched caster sets
- Minimal disruption to clinical operations
Reactive replacement, by contrast, happens after failure already affects operations—and the costs are harder to absorb:
- Emergency procurement at premium pricing
- Staff overtime for urgent installation
- Lost bed availability during repair
- Potential incident reports if failure occurs during patient care
The simplest way to stay ahead: attach caster inspections to maintenance cycles already on the calendar—annual biomed equipment checks or quarterly housekeeping audits. No new scheduling required, and no caster failures that catch a shift by surprise.
What Happens When Caster Replacement Is Delayed Too Long
Patient Safety Outcomes
A caster that fails suddenly during patient transfer—rather than degrading gradually—creates immediate fall risk. A broken housing, seized swivel, or failed brake removes a key safety margin precisely when it's most needed. Gradual wear lets staff unconsciously compensate over time. Sudden failure during a lateral transfer or bed-to-chair move does not — it produces uncontrolled bed movement when the patient is most exposed.
Staff and Liability Costs
Staff pushing beds with high-resistance or malfunctioning casters face elevated risk for back, shoulder, and wrist strain. These injuries carry direct costs in workers' compensation claims, with healthcare back injuries totaling approximately $20 billion annually in direct and indirect costs.
Documented equipment failures on incident reports also create legal exposure. When fall incidents or staff injuries list "malfunctioning bed casters" as a contributing factor, the facility's preventive maintenance records become discoverable evidence in litigation.
Floor and Equipment Damage
Worn or flat-spotted casters leave drag marks, gouges, and scuff marks on vinyl, epoxy, and specialty flooring. Lifecycle cost analysis shows VCT flooring costs $112.80/sf over 50 years versus $69.80/sf for resinous flooring, with wheeled traffic rated 5/5 importance for patient treatment areas.
The compounding effect is worth noting:
- Drag damage accelerates floor degradation, pushing facilities toward the higher end of lifecycle cost projections
- Floor refinishing and patching costs consistently outpace the cost of the casters that caused the damage
- Replacing worn casters proactively is one of the lowest-cost interventions in a facility's maintenance budget

Hospital Bed Caster Buyer's Guide for Facilities
Load Capacity and Mount Compatibility
Replacement casters must match both the bed's mounting system and carry appropriate load ratings with safety margin:
Mounting Systems:
- Grip-ring stems (friction-fit expansion)
- Threaded stems (screw-in attachment)
- Top plate (bolt-down mounting)
- Expanding socket (compression-fit)
Humphries Casters supplies all four mount types compatible with Hill-Rom, Stryker, Joerns, Invacare, and other major bed manufacturers.
Load Rating Calculation:
ICWM/ANSI static testing requires casters to withstand 4 times rated load capacity without failure. For dynamic operating conditions, use the three-caster rule: divide total weight by 3 (not 4) to account for uneven floors where one caster may temporarily lift.
Example: A bed rated for 500 lb patient capacity, plus 100 lb accessories and 385 lb frame weight = 985 lb total. Divided by 3 = 328 lb minimum per-caster rating. Select casters rated for 350-400 lb to maintain safety margin.
Selecting casters rated at exact maximum expected load (rather than with buffer above it) leads to premature failure.
Wheel Material Selection Guide
| Material | Best For | Key Advantages | Considerations |
|---|---|---|---|
| TPR | Patient rooms, recovery wards | Quietest operation, excellent floor protection, non-marking | Lower load capacity, moderate chemical resistance |
| Polyurethane | ICU, bariatric beds, high-traffic areas | Superior load-bearing, excellent chemical resistance, abrasion-resistant | Louder than TPR, higher cost |
| Stainless Steel Housing | Wet environments, autoclave areas | Complete corrosion resistance, longest mechanical life | Loudest operation, can damage flooring |
WHO recommends hospital sound levels not exceed 30 dB in general areas and 35 dB in patient rooms, yet actual ICU measurements consistently exceed 45 dBA. TPR casters minimize rolling noise contribution in environments already failing to meet acoustic guidelines.
For units running intensive disinfection protocols, polyurethane holds up better against cleaning chemicals, oils, and solvents than rubber or TPR.

Features That Matter Most in Clinical Settings
Sealed precision bearings: Resist cleaning fluid penetration and extend service life in high-wash environments. Request IP (Ingress Protection) ratings from manufacturers.
Brake systems: Match the bed's existing system — mixing brake types creates operational confusion.
- Total lock (secures wheel and swivel simultaneously) for stationary procedures
- Directional lock (locks swivel only) for straight-line corridor navigation
Noise level: For ICU and recovery ward applications, specify near-silent operation. Request product samples before bulk ordering to evaluate in your environment.
Compliance: Confirm replacement casters maintain IEC 60601-2-52 compliance for adult medical bed basic safety and essential performance requirements.
Humphries Casters offers product trials and samples so procurement teams can evaluate fit before committing to a bulk order. The company's warranty extends beyond standard manufacturer coverage — including exchanges and refunds when products don't meet operational requirements.
Frequently Asked Questions
When to replace caster wheels?
Replace caster wheels when visible tread degradation, audible bearing noise, brake malfunction, or structural damage appears. Even without visible failure, high-use hospital beds warrant inspection every 3-6 months with preventive replacement on a condition-based schedule rather than waiting for complete failure.
What are casters on a hospital bed?
Casters are wheeled assemblies at the base of hospital beds that allow rolling, steering, and locking in place. Each unit includes a wheel, swivel housing, bearing system, and brake mechanism — with central locking systems tying all four casters to a single pedal.
What are the common problems with castors?
The most frequent issues include worn or cracked wheel treads reducing smooth movement, bearing failure causing grinding noise or wobble, brake mechanisms that stick or fail to engage compromising patient safety, corroded housings from chemical exposure, and flat spots from prolonged stationary loading creating vibration during transport.
How do I know what size casters I need?
Correct size is determined by the bed's existing mounting socket dimensions (stem diameter and type), required load capacity (total weight divided across four casters plus safety margin), and wheel diameter suited to your floor surface. Contact the bed manufacturer or measure the existing caster stem before ordering.
How often should a hospital bed be replaced?
Hospital bed frames typically last 10-15 years, but casters are consumable components that wear out much sooner. Replacing casters every 18-36 months based on condition is far more cost-effective than waiting for complete failure — or replacing the bed.
Can I replace just one caster or do all four need replacing at once?
A single failed caster can be swapped in an emergency, but replacing all four at once is strongly recommended. Mismatched casters create uneven load distribution and inconsistent braking, which accelerates wear on the remaining units.