Introduction
In a hospital, a caster failure is a patient safety event. A stretcher wheel seizing mid-transport, a bed brake failing during transfer, or a medication cart tipping over can cause injury, equipment damage, and real liability exposure.
Yet many facilities still spec casters by guessing weight or copying whatever was on the previous cart—leading to premature failures, costly replacements, and preventable safety incidents.
Getting load capacity right in a hospital requires more than dividing total weight by four casters. It means understanding static versus dynamic ratings, hospital-specific safety factors, and the unique demands of healthcare environments: shift-length use, chemical disinfection exposure, uneven floor transitions, and continuous rolling cycles across 24/7 operations.
This guide covers the calculation formula, the factors that affect ratings in clinical settings, load requirements by equipment type, and how to avoid the most common specifying mistakes that put staff and patients at risk.
Key Takeaways
- Caster load capacity is the maximum safe working load per caster—hospitals must use the dynamic (rolling) rating, not just the static one
- Use this formula to size correctly: total weight ÷ (number of casters − 1) to account for uneven floors and real-world load shift
- Always apply a safety factor of 25–33% minimum above the calculated per-caster load; continuous-use hospital equipment often warrants higher margins
- Wheel material, diameter, floor type, and chemical exposure all affect real-world capacity — a sufficient rated number on paper isn't the whole picture
- Specification varies by equipment type: hospital beds, crash carts, and heavy diagnostic equipment each carry different load profiles and risk levels
What Is Caster Load Capacity?
Caster load capacity is the maximum weight a single caster can safely support during use. The catch: manufacturer ratings are established under controlled laboratory conditions—smooth floors, standard temperatures, intermittent use—conditions that rarely exist in a working hospital. Spec from the published number without adjustment, and you're likely undersizing.
Static vs. Dynamic Load Ratings
Static load capacity refers to the weight a caster can hold while stationary, important for parked beds and idle carts. Dynamic load capacity is the weight a caster can handle while rolling under normal operating speed—typically measured at 3 mph for 10,000 feet under ICWM testing protocols. Dynamic ratings are typically lower than static ratings and represent the operationally relevant number in hospitals where equipment moves constantly across shifts.
Dynamic capacity typically runs 50–75% of static capacity, depending on wheel material:
- Soft-compound rubber: approximately 50–60% of static
- Polyurethane on iron: approximately 60% of static
- Cast iron and forged steel: approximately 70–75% of static
Shock load capacity covers sudden impacts—rolling over elevator thresholds, door strips, floor transitions. In a hospital, equipment crosses these dozens of times per shift. Ignore shock de-rating and even a correctly-specced caster can fail prematurely.
Why Hospital Environments Change the Calculation
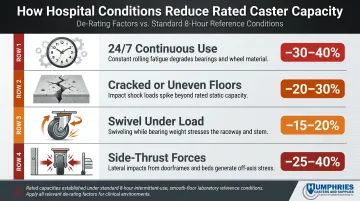
Hospital conditions systematically erode the published rating. Continuous 24/7 movement, chemical disinfectant exposure, elevator gaps, threshold strips, and mixed flooring all reduce real-world effective capacity. Per engineering guidance from CasterHQ, common de-rating factors include:
- 24/7 continuous use: reduces effective capacity by 30–40% versus 8-hour-per-day reference
- Cracked or uneven floors: 20–30% de-rate
- Swivel under load: 15–20% de-rate
- Side-thrust forces (common when turning): 25–40% de-rate
How to Calculate the Right Caster Load for Hospital Equipment
Guessing or using round numbers puts staff and patients at risk — and shortens caster lifespan. Follow this step-by-step formula used by procurement professionals and engineers:
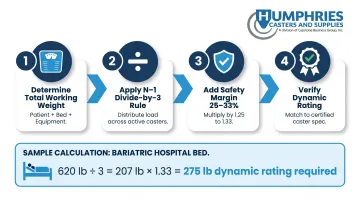
Step 1 — Determine Total Working Weight
Total working weight includes:
- Empty weight of the equipment or cart
- Maximum payload it will carry (supplies, instruments, IV bags)
- For hospital beds and stretchers: maximum anticipated patient weight
For facilities serving bariatric patients, factor in appropriate weight ranges. Medicare/insurer thresholds cite heavy-duty as >350 lb and extra heavy-duty as >600 lb patient weight.
Step 2 — Apply the Divide-by-Three Rule
Divide total weight by (number of casters − 1) rather than the full caster count. On uneven floors, elevator transitions, or threshold gaps common in hospitals, at least one caster is often slightly off the ground and not bearing load—making the remaining casters carry the full weight.
For a 4-caster setup, divide by 3. This N−1 sizing method is recommended by multiple caster engineering resources to account for real-world uneven distribution.
Step 3 — Add the Safety Margin
The result from Step 2 is the minimum per-caster load. Hospitals should select casters rated at least 25–33% above this minimum for standard equipment. Equipment in continuous use or subjected to chemical exposure warrants higher margins.
According to industry engineering guidance, a safety factor of 1.25x applies for normal use, with 1.35x recommended where routine impacts exist.
Step 4 — Verify the Dynamic Rating, Not Just the Static
Caster spec sheets typically display the static rating prominently. Procurement staff must request or look up the dynamic (rolling) load rating — the figure that reflects real rolling conditions, and typically runs 60–75% of the static number. Specifying by static rating alone leads to under-spec'd casters that fail prematurely.
Here's how those four steps play out in a real procurement scenario.
Worked Example: Standard Hospital Bed
Equipment: Standard hospital bed
Bed frame + mattress: 120 lb
Maximum patient weight: 500 lb (bariatric capacity)
Total working weight: 620 lb
Calculation:
620 lb ÷ 3 casters = 207 lb per caster (minimum)
Apply 33% safety factor:
207 lb × 1.33 = 275 lb dynamic rating required per caster
For this application, specify casters with a minimum 275 lb dynamic rating to ensure safe operation under real-world hospital conditions.
Factors That Affect Caster Load Ratings in Hospital Settings
Two casters with the same rated number can perform very differently in a hospital depending on wheel material, size, environment, and use pattern. These variables must be factored into the spec process.
Wheel Material
Wheel material directly impacts load-bearing performance:
- Polyurethane: 5-inch wheels typically rated 500–1,500 lb; excellent floor protection; temperature range −20°F to 180°F.
- Nylon (glass-filled): 5-inch wheels rated 800–2,500 lb; low rolling resistance but poorer floor protection; temperature range −40°F to 200°F.
- Phenolic: 5-inch wheels rated 500–1,000 lb; heat tolerant up to 325°F continuous; harder on floors and creates noise concerns.
- TPR (thermoplastic rubber): 5-inch wheels rated 200–500 lb; quiet operation, shock-absorbing, non-marking; good floor protection but lower capacity.
Chemical resistance is critical: According to material compatibility guides, polyolefin rates "Excellent" for sodium hypochlorite exposure, while many elastomers and polyurethanes degrade under oxidizing bleach solutions. For hydrogen peroxide 10% exposure, nylon glass-filled and polyolefin rate Excellent, while rubber/TPR often rate poorly due to softening.
Wheel Diameter and Tread Width
Larger wheel diameters improve load capacity and make it easier to roll over thresholds and elevator gaps — a real factor in hospitals where equipment passes through multiple room transitions daily. Wider tread widths distribute weight over a larger contact surface, which also increases effective capacity.
Within the same caster model family, stepping up in diameter or tread width can raise load capacity without changing the mounting hardware. That makes it a low-disruption upgrade when a facility's load requirements increase.
Floor Type and Surface Conditions
Hospitals typically span several floor types across zones — LVT (luxury vinyl tile), VCT (vinyl composition tile), epoxy-sealed concrete, and carpet — and each one changes the rolling resistance and shock loading a caster experiences.
Hard floors roll more efficiently but amplify vibration. Uneven joints, threshold strips, and elevator plate edges act as repeated impact events that reduce a caster's effective capacity (de-rate it) over time. Soft or rough surfaces compound this by forcing wheels to work harder on every pass.
Frequency and Duration of Use
Most caster ratings assume an 8-hour intermittent duty cycle. Hospital environments run 24/7, and high-traffic equipment — crash carts, transport stretchers, nurse carts — far exceeds those rolling-cycle assumptions.
According to CasterHQ engineering guidance, continuous 24/7 use reduces effective capacity by 30–40% compared to standard 8-hour reference conditions. That gap is significant enough to move a caster into the next capacity tier when speccing for clinical use.
Brake and Swivel Load Interaction
Two additional de-rates apply in most hospital configurations:
- Swivel vs. rigid: Swivel casters de-rate 15–20% compared to rigid ones because rotating under load stresses the raceway. Swivel-heavy setups need this factored in from the start.
- Total-lock brakes: Locking both wheel and swivel creates static load stress points — particularly relevant for parked beds where patients remain on them for hours. Soft-tread wheel types are most sensitive to this and carry lower static load limits as a result.

Load Capacity Requirements by Common Hospital Equipment Type
Applying a single load rating across all hospital equipment is a major procurement error. Different equipment types have fundamentally different weight profiles and failure risk levels.
Hospital Beds and Stretchers
Typical load profile: bed frame weight + mattress weight + patient weight (standard and bariatric ranges)
Example specifications from major OEMs:
- Hillrom/Baxter Centrella Smart+: Safe Working Load 650 lb; patient weight range 70–500 lb; 5-inch central-locking casters
- Stryker MV3 bariatric bed: Safe Working Load up to 1,102 lb
Typical hospital mattresses weigh 15–40 lb; bariatric foam mattresses weigh 35–40 lb.
Per-caster implications: For a standard bed with 500 lb patient capacity and 120 lb bed/mattress weight, total working weight is 620 lb. Using the N−1 formula: 620 ÷ 3 = 207 lb minimum per caster before safety factors. After applying a 33% safety margin, specify casters with 275 lb dynamic rating minimum.
Bariatric applications require higher per-caster ratings — often double the standard bed spec. Central locking casters also experience concentrated static load stress when beds are left in place for extended periods, so static capacity matters as much as dynamic rating here.
Medical Carts (Crash Carts, Medication Carts, IV Poles)
Total loads are lower than beds, but these carts move constantly — during rounds, emergencies, and restocking. That frequency shifts the spec priorities:
- Dynamic load capacity
- Rolling resistance (reducing nurse fatigue)
- Durability over very high rolling cycle counts
Crash carts in emergency departments face more abuse and threshold crossings than any other cart type. Even though payload may be modest (100–200 lb total), the continuous movement and shock loading from threshold crossings warrant casters with robust dynamic ratings and impact resistance.
Heavy Diagnostic and Imaging Equipment
Ultrasound machines, portable X-ray units, C-arms, and mobile anesthesia carts represent the highest load demands outside of fixed imaging rooms.
Representative equipment weights:
- Mobile C-arms: Siemens Cios Select C-arm: 605 lb; monitor cart: 330 lb
- Portable X-ray: GE Optima XR220amx: approximately 1,000 lb
- Ultrasound systems: GE LOGIQ S8: 187 lb; GE LOGIQ E10: 278 lb
- Anesthesia carts: Drager Atlan A350: 298 lb base setup
Per-caster calculation example: A 605 lb mobile C-arm on 4 casters implies 605 ÷ 3 ≈ 202 lb dynamic per caster before safety factors. Applying a 33% margin yields 270 lb dynamic rating minimum per caster.
These units are heavy but moved infrequently. That shifts the priority toward static load capacity and leveling caster options rather than rolling cycle durability. A caster failure under a 1,000 lb portable X-ray unit is a serious staff injury event, not just a maintenance call.

Specialty Environments (MRI, Sterile Processing, Bariatric)
These three environments each impose constraints beyond load rating alone — material compatibility, temperature resistance, and magnetic safety all affect caster selection.
MRI suites require non-ferrous casters regardless of load rating. MRI safety guidance emphasizes strict zone control and prohibition of ferromagnetic items. MRI-conditional designs use glass-filled nylon housings and 316 stainless components to meet this requirement without sacrificing load capacity.
**Sterile processing and autoclave environments** require specific material compatibility. High-temperature autoclavable casters can withstand sterilization temperatures up to 275°F with stainless bearings and heat-resistant wheel compounds.
Bariatric care units need the highest load ratings with soft-tread wheels to protect floors and reduce patient discomfort. These specialty environments often require caster consultation rather than catalog selection because standard load-rated options may not meet the full specification.
Common Load Capacity Mistakes in Hospital Procurement
Most hospital caster failures trace back to a handful of predictable specifying errors — all of them avoidable.
Mistake 1: Dividing by 4 Instead of 3
Dividing total weight by the full caster count (rather than casters minus one) produces under-rated casters that fail ahead of schedule. Hospitals cross thresholds, elevator gaps, and floor-type transitions constantly. Any time one caster lifts off the ground, the remaining three carry the entire load.
Impact: Premature bearing wear, wheel deformation, and brake failure.
Mistake 2: Using the Static Rating as the Working Number
Selecting casters based on the headline static number without checking the dynamic rating means the caster is effectively under-spec'd for actual rolling use. Dynamic ratings are typically 60–75% of static ratings, depending on wheel material.
Impact: Tread failure and bearing wear within months, especially under continuous hospital use patterns.
Mistake 3: Ignoring Chemical Exposure and Material Compatibility
A caster perfectly rated for the load may still fail prematurely if the wheel compound degrades from exposure to hospital-grade disinfectants.
Most resistant materials:
- Polyolefin and nylon glass-filled: Excellent resistance to sodium hypochlorite and hydrogen peroxide
- Polyurethane on aluminum cores: Good resistance in most disinfectant environments
Least resistant materials:
- Rubber/TPR compounds: Poor resistance to oxidizing agents; soften and degrade under bleach and peroxide exposure
The result is wheel cracking, tread separation, and load capacity loss — even on correctly spec'd casters.
How Humphries Casters Can Help
Humphries Casters is a specialist supplier with direct experience serving hospitals—including several facilities ranked #1 in their specialties or regions—as well as the top long-term care organizations in America. Since 1988, the company has built its reputation on sourcing specifications and solving problems that standard distributors routinely turn away.
Specific ways Humphries supports hospital procurement teams:
- Sources hard-to-find specifications: central locking mechanisms, custom stem configurations, high-temperature and corrosion-resistant designs, and specialty wheel materials
- Provides evaluation samples so hospitals can test casters under real conditions before committing to a full fleet order
- Arranges onsite demonstrations and training for larger equipment—such as hospital bed movers—to ensure proper installation and operation
- Offers blanket orders and bulk pricing structured around hospital procurement cycles, with flexible stocking and delivery options
- Extends warranty protection beyond standard manufacturer coverage, often covering a broader range of failure conditions

Facilities managers and procurement staff can reach Humphries directly at 800.733.4758 or Service@HumphriesCasters.com. Bring your weight data and equipment details—the team will spec the right caster for each application.
Frequently Asked Questions
How to calculate caster load?
Caster load is calculated by dividing the total working weight (equipment + maximum payload, including patient weight for beds) by the number of casters minus one. Then add a safety margin of at least 25–33% above that result to account for real-world conditions and continuous use.
How do I know what size casters to use?
Size selection involves both wheel diameter (larger helps with floor transitions and increases capacity) and tread width (wider distributes load better). The hospital's floor type and equipment weight profile together determine the right combination. Consult engineering guides or a caster specialist for high-load applications.
What is the load capacity of casters?
Load capacity is the maximum safe working load per caster at a given duty cycle. This figure comes in static (stationary) and dynamic (rolling) versions. The dynamic rating is the relevant number for most hospital equipment that moves regularly.
What is the difference between static and dynamic load capacity?
Static capacity is what a caster can hold at rest without deformation. Dynamic capacity is what it can safely roll under repeatedly—dynamic ratings are typically 60–75% of static and are the number that matters most when specifying casters for hospital equipment.
What safety factor should I use for hospital casters?
A minimum 25–33% safety buffer above the calculated per-caster load is standard. Continuous-use and chemical-exposure environments warrant a higher margin. For high-stakes equipment like bariatric beds, work directly with a caster specialist to confirm the right rating.
How often should hospital casters be inspected or replaced?
Inspect casters on active hospital equipment at least quarterly for tread wear, swivel resistance, brake performance, and bearing noise. High-traffic equipment like crash carts and transport stretchers may need inspection more frequently and replacement within 2–4 years depending on usage intensity.